Performance-based pricing for pharmaceuticals
Purchasers, manufacturers explore new pricing models
As the cost of specialty drugs surges-and even prices for generics have risen-purchasers are working closely with manufacturers to sort out new ways to pay for certain medications.
“Most everyone agrees that drug pricing is an issue that has been exacerbated by specialty drugs entering the market at very high price points when most are thinking in terms of traditional branded chemical drugs,” says Randy Vogenberg, PhD, principal, the Institute for Integrated Healthcare in Greenville, South Carolina.
An emerging model
Novartis’ new drug for treating heart failure, Entresto, is an example of a medication ripe for performance-based pricing. A double-blind, random trial with 8,442 adults revealed a lower rate of death from cardiovascular causes (Entresto, 21.8% vs. 26.5% for enalapril) and a relative risk reduction in hospitalizations for heart failure of 21% for those taking Entresto as compared to enalapril, a generic ACE inhibitor and common treatment for high blood pressure and congestive heart failure. The trial ended early after a median follow-up of 27 months because Entresto had indicated significant risk reduction in death at that point, according to an article in the Sept. 11, 2014 issue of The New England Journal of Medicine. Enalapril costs far less than Entresto, which is pinned at $12.50 per patient per day.


Novartis has been batting around some ideas for a performance-based pricing model to ensure there is less sticker shock for the new drug-offering upfront discounts with bonus payments later if Entresto lives up to its promise of fewer hospitalizations and lower associated costs, according to recent news articles.
Novartis might also add on services, such as developing a remote monitoring device to be used in the home to measure patient status before hospitalization becomes necessary.
“We have reached out to payers to discuss potential contracting models linked to approved clinical outcomes as outlined in the U.S. prescribing information for Entresto. Some payers have shown interest, and we are proceeding with further evaluation to ascertain an appropriate and mutually agreeable contract framework,” according to the company. “Novartis wants to be part of the solution by advancing outcomes-based contracting on Entresto."
Next: Indication-specific drug pricing
Indication-specific drug pricing
Sometimes a drug designed to treat two different conditions proves to be more effective for one indication over another. That is one impetus behind Express Scripts’ decision to deploy a performance-based pricing model for certain drugs. Tarceva (Roche Holding AG and Astellas Pharma Inc.), a drug indicated to treat both lung and pancreatic cancer, is its first test case.
Express Scripts found that using Tarceva for lung cancer resulted in an average 5.2 months longer survival rate versus chemotherapy; however, results of the effect of Tarceva on pancreatic cancer indicated that the survival rate of these patients only increased by two weeks versus a placebo.



Steve Miller, MD, chief medical officer, Express Scripts, says the cost of the drug for pancreatic cancer should be lower than for patients with lung cancer. He calls the approach “indication-specific pricing”-paying claims based on the indication for which the medication is used.
Miller notes that Express Scripts distinguishes between performance- and outcomes-based models, saying the latter allows little accountability for patients who choose not to take a drug or stop because of side effects, leading to more complicated pricing.
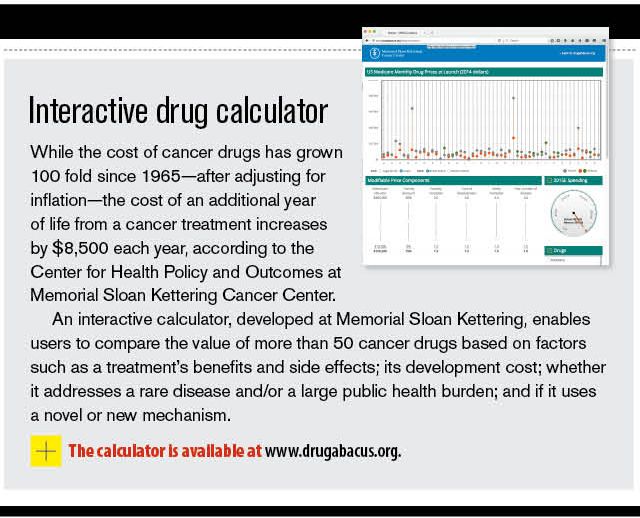
The PBM relies on the Center for Health Policy and Outcomes at Memorial Sloan Kettering Cancer Center, as well as on the Institute for Social and Economic Research, as independent third parties reviewing the economics of certain drugs.
“We walk a tightrope-trying to reward innovative drugs while ensuring that we keep the prices affordable for patients,” Miller says. “We don’t want to overpay for a drug that is only marginally better than an alternative.”
Miller anticipates extending the performance-based model to pricing other specialty drugs, such as those for multiple sclerosis and immunosuppressants.
Next: Determining value
Determining value
Performance-based models could come in different flavors-basing prices on how well a drug reduces hospitalizations and readmissions, if it extends life or how well it performs against a competitive drug.



MartinThere’s another way to determine value, says Sarah Martin, vice president and senior pharmacy consultant, Lockton Benefit Group. A drug could be considered more valuable if it has fewer side effects and is easier to take or administer, Martin says.
“However value is defined, what matters most is that any cost savings associated with a PBM’s efforts to establish value-based or performance-based contracts with pharmaceutical manufacturers must trickle down to health plans, employers and the patients who ultimately bear the cost of the drug and are the beneficiaries of its value,” she adds.
Martin also believes that it is important to view cost and value holistically by paying attention to both medical and pharmacy costs.
“We’ll see a trend in the direction of performance-based models. Oncology is the biggest threat from a cost perspective when we consider drugs in the pipeline,” she says. “As a society, we will not be able to bear the costs unless the payment models are redefined. Most stakeholders in the PBM and pharmacy industry have incentives that aren't aligned with the ultimate payer, so these performance-based models could be an effective way to address those challenges, assuming the right models are developed.”









David Calabrese of OptumRx Talks New Role, Market Insulin Prices and Other Topics 'On His Mind'
April 13th 2023In this month’s episode of the "What's On Your Mind podcast," Peter Wehrwein, managing editor of MHE connects with the now Chief Clinical Officer of OptumRx Integrated Pharmacies, David Calabrese. In this conversation, David touches on his transition in January as OptumRx’s former chief pharmacy officer and market president of health plans and PBMs to his new role as Chief Clinical Officer where he now focuses more on things such as specialty pharmacy to home delivery — with an overall goal of creating whole-patient care. Throughout the conversation, Calabrese also touched on the market’s hot topic of insulin prices and behavioral health services within the OptumRx community, among other topics.
Listen

Upended: Can PBM Transparency Succeed?
March 6th 2024Simmering tensions in the pharmacy benefit management (PBM) industry have turned into fault lines. The PBMs challenging the "big three" have formed a trade association. Purchaser coalitions want change. The head of the industry's trade group says inherent marketplace friction has spilled over into political friction.
Read More

Briana Contreras, editor of Managed Healthcare Executive, spoke with Nancy Lurker, CEO and president of EyePoint Pharmaceuticals. Nancy shared a bit about EyePoint and how the organization’s innovative therapies are addressing patient needs through eye care, and most importantly, she addressed C-Suite positions like the CEO role. Nancy shared advice for those seeking to reach the CEO level, especially toward women in healthcare and other roles, and what it takes to run a biopharma company.
Listen

The deliberate disconnection of Change Healthcare to ring fence a cyberattack entered its seventh day today. Prescribers are finding ways to get pharmacy claims processed, and UnitedHealth Group says disruption to the dispensing of prescriptions has been minimal. But independent pharmacies want more information and protection from financial consequences from pharmacy benefit managers.
Read More


