
News|Articles|August 1, 2024
Adults Should be Part of Early Screening Efforts for Type 1 Diabetes
Author(s)Denise Myshko
As many as 40% of people with type 1 diabetes are unaware that they have the disease.
Advertisement
Early screening for type 1 diabetes is critical for preventing serious disease, Andrew Cagle, M.D., senior medical director, Autoimmune Diabetes and T1D Immunotherapy and Medical Affairs at Sanofi, said in a recent interview.
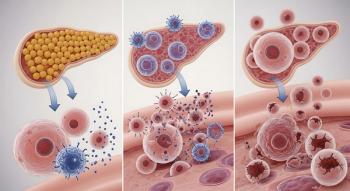
Type 1 diabetes is an autoimmune disease that affects about 2 million Americans, about 5% to 10% of all diabetes cases, according to the Centers for Disease Control and Prevention (CDC). In type 1 diabetes, the pancreas does not make insulin.
But as many as 40% of people with type 1 diabetes are unaware that they have the disease. Risk factors include having a parent or sibling with the disease.
A blood test can be done to screen for autoantibodies, which are not present in people with type 2 diabetes.
“When I was practicing, we were using the test to screen for type 1 diabetes to confirm the diagnosis, particularly in the adolescent age group when diabetes is starting to emerge,” Cagle said. “Now we’re using it in the field to screen for type 1 diabetes before symptoms take place. And, hopefully, we can make that diagnosis before people get really sick.”
He said screening needs to include adult populations as well to avoid the potential misdiagnosis of type 2 diabetes, which has a different standard of care. People of any age can get type 1 diabetes, although it usually develops in children, teens and young adults.
“It’s now recommended that at minimum family members or people with a family history of autoimmune diseases or who have autoimmune diseases themselves be screened for the diabetes antibodies so we can make the diagnosis.”
Currently, there is no recommendation for general screening for type 1 diabetes. But recently, a group of international diabetes organizations released a guidance in support of monitoring patients who at risk for type 1 diabetes. Currently, screening for islet autoantibodies is done for those with a first-degree relative with the disease. But the authors pointed out that up to 90% of people who develop type 1 diabetes are not part of at-risk groups.
The guidance provides recommendations for specialists to work with primary care physicians to monitor at-risk children. But the guidance also recommends that monitoring of at-risk adults is even more important. Although progression of type 1 diabetes is slower in adults, adults with multiple autoantibodies can develop clinical diabetes.
“In order to prevent people from getting really sick, we can’t limit screening to just the people with a family history,” Cagle said. “That’s a challenge, because that’s asking our partners in primary care to a participate in the screening, and they’re so busy nowadays. That’s a barrier and we need more education to help with that.”
The costs for early screening may be offset by reduction in costs related to diabetic ketoacidosis events. In one study
More recently, Cagle and his colleagues at Sanofi found increased healthcare use among intially diagnosed children with type 1 diabetes, especially among those with Medicaid.
In study, they aimed to examine clinical and healthcare resource utilization burden of type 1 diabetes among real world patients. They conducted a retrospective analysis of Merative MarketScan data from Jan. 1, 2015, to June 30, 2018, among nearly diagnosed children with type 1 diabetes up through the age of 17.
The study was
In this analysis, healthcare resource utilization, including diabetic ketoacidosis events, and type 1 diabetes-related events, such as outpatient and inpatient care and emergency room (ER) visits, were analyzed, and the findings were segregated based on health plan type.
They identified 4,092 patients enrolled in the commercial health plans and 1,153 patients in Medicaid. They found that pediatric patients younger than 5 years age enrolled in Medicaid experienced higher rates of diabetic ketoacidosis events around initial clinical diagnosis of type 1 diabetes compared with those covered by commercial plans.
During the post-diagnosis follow-up period, diabetic ketoacidosis events were 2.5 times higher in patients with type 1 diabetes who have Medicaid coverage, which may indicate a disparity in care provided to patients covered under Medicaid.
Newsletter
Get the latest industry news, event updates, and more from Managed healthcare Executive.
Advertisement
Related Content
Advertisement


Latest CME



















Advertisement
Advertisement
Trending on Managed Healthcare Executive
1
7 things you need to know about the PBM reforms signed into law this week
2
What exactly is managed care today?
3
TrumpRx launches; some experts question its long-term value
4
PBM reform. It has finally happened
5